
 The Doctor Is In!
The Doctor Is In!
 The Doctor Is In!
The Doctor Is In!Q & A with Dr. John Frederick Payne, MD
Reproductive Endocrinologist & PREG Partner
ICSI and other advances in the Embryology Lab
How Does the Embryology Lab Work in Fertility Treatment?
Obviously, before we get to the lab and they do their part we have to do the in-vitro fertilization or embryo transfer so that we can begin the fertilization process. Eggs and sperms end up and are put together through standard insemination, or we save the eggs in a culture media and incubate them and fertilize to grow embryos. It takes 5-6 days to generate them or cryopreserve them for frozen transfer which is becoming more common than fresh embryos.
What Kind of Testing is Done on the Front End?
 They will undergo PGT (Preimplantation genetic testing) which examines embryos during IVF before transfer to a woman’s uterus for the screening of a broad range of genetic problems that can cause implantation failure, miscarriages, and birth defects in a conceived child. PGT-A is genetic testing for aneuploidy to help us select which embryos created through IVF have the most positive outcomes for pregnancy and a healthy baby. Basically we are testing to identify the embryos that have a normal number of chromosomes (euploid) and those that have an abnormal number known as aneuploidy. There can be a genetic normal, one missing a chromosome or otherwise abnormal, and would not be implanted. We weed out the abnormal ones to increase the chances of pregnancy for embryo transfers. We are lowering the risk for conceivers for miscarriage, etc. 75-80% of pregnancy failures are due to abnormal embryos.
They will undergo PGT (Preimplantation genetic testing) which examines embryos during IVF before transfer to a woman’s uterus for the screening of a broad range of genetic problems that can cause implantation failure, miscarriages, and birth defects in a conceived child. PGT-A is genetic testing for aneuploidy to help us select which embryos created through IVF have the most positive outcomes for pregnancy and a healthy baby. Basically we are testing to identify the embryos that have a normal number of chromosomes (euploid) and those that have an abnormal number known as aneuploidy. There can be a genetic normal, one missing a chromosome or otherwise abnormal, and would not be implanted. We weed out the abnormal ones to increase the chances of pregnancy for embryo transfers. We are lowering the risk for conceivers for miscarriage, etc. 75-80% of pregnancy failures are due to abnormal embryos.
What Are you Testing For?
PGT-A has become a standard part of the IVF cycle around the world. In certain situations it is used to help diagnose and alleviate hidden causes of infertility in women 35+ years of age; Couples with unexplained infertility; People who have experienced a previous IVF failure; women with recurring miscarriages; and women who have had an abnormal pregnancy previously with a child with a genetic condition as well as women of advanced age having a baby with Downs and/or Turner syndromes.
We are looking for things like mutations in single genes (monogenic disorders) that include SMA (spinal muscular atrophy), cystic fibrosis, and other conditions. We select embryos that are not at an increased risk of developing a single gene disorder. We are increasing the chances of a healthy pregnancy and the ultimate delivery of a healthy baby and mother.
How Has This Changed in IVF Treatment?
Historically people would want to have the testing after having the child and then we would go back and test the parents. Now we have more expanded carrier screening where we can screen for 200-300 diseases. They could be carriers or transmitters. There is a 1/20 chance couples will match up for the same disease. Through aneuploidy testing, we can identify missing or extra chromosomes that could cause a miscarriage or life-altering disorder. We are selecting a normal embryo faster than random selection by the old form of grading and looking under the microscope in an embryo “beauty” contest. We can now select the highest grade and work our way down. Single embryo transfers help eliminate multiple gestations and keep success rates higher which allows us to be more efficient and present less risk to the woman of trying to carry multiple pregnancies and the complications that can accompany multiple gestations.
What is ICSI & Why Is It Recommended?
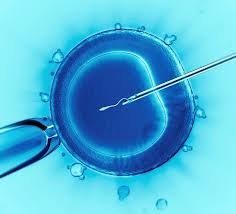
 It is called Intracytoplasmic sperm injection. The embryologist can take a single sperm sample that is moving and looks normal. Then they aspirate it into a little injection needle on the ICSI while holding the egg in place on the other side and inject the needle into the middle of the egg. The sperm is injected inside the egg which gives the highest probability for fertilization, especially if there is a lower sperm count, movement, other male-factors, or in unexplained fertility where she isn’t getting pregnant. We are increasing the chances and removing as many obstacles as possible to maximize success.
It is called Intracytoplasmic sperm injection. The embryologist can take a single sperm sample that is moving and looks normal. Then they aspirate it into a little injection needle on the ICSI while holding the egg in place on the other side and inject the needle into the middle of the egg. The sperm is injected inside the egg which gives the highest probability for fertilization, especially if there is a lower sperm count, movement, other male-factors, or in unexplained fertility where she isn’t getting pregnant. We are increasing the chances and removing as many obstacles as possible to maximize success.
So five things have to happen to attempt conception:
Ovulation
1 or two fallopian tubes are open
The presence of sperm
Fertilization in the fallopian tubes
The embryo is down the fallopian tubes, implanted or attached to the uterus
What Are You Able to Do with These Microscopes?
 These high powered microscopes have micromanipulators and suction to hold an embryo in place to help fertilize the egg as it grows. The laser attachments can make a pinpoint opening in the embryo to get cells as they ooze out. 4-6 are separated with the laser pulling apart from the rest of the embryo and the cell mass that is going to be the baby is not touched in the process. We freeze the embryos and two weeks later get results on which are normal, or ineffective. We compare this to the uterus as we wait to get the uterus back to the same spot it was five days before by using a catheter at the top of the uterus as if it had been fertilized into the fallopian tubes. 12 days later we are ready for a pregnancy test.
These high powered microscopes have micromanipulators and suction to hold an embryo in place to help fertilize the egg as it grows. The laser attachments can make a pinpoint opening in the embryo to get cells as they ooze out. 4-6 are separated with the laser pulling apart from the rest of the embryo and the cell mass that is going to be the baby is not touched in the process. We freeze the embryos and two weeks later get results on which are normal, or ineffective. We compare this to the uterus as we wait to get the uterus back to the same spot it was five days before by using a catheter at the top of the uterus as if it had been fertilized into the fallopian tubes. 12 days later we are ready for a pregnancy test.
What About Today’s Lab Standards & Quality?
Years ago the technology and media weren’t there to do what we do now. We now have the ability to have the media, embryos, etc. to live in proper temperatures, correct oxygen, and nitrogen mixtures while being continually monitored with multiple alarms and safety protocols. When you stop and think about it’s .amazing at what has to be done outside the body to do what a woman in a natural pregnancy does inside the body….I can’t make anyone get pregnant but now we can set the optimal parameters and place an embryo in the perfect place but it has to be normal and the uterus has to be acceptable, timing right, and some luck, and by God’s grace we have a pregnancy.
What Has Changed?
 The ability to grow embryos in the lab has increased through the development of ICIS in 1995 which now allows us to treat in the middle of the process. The old way with standard insemination takes eggs retrieved in a culture dish and puts a sperm concentration in it in the same drop to fertilize. The problem is it didn’t work if there was a significant male- factor such as low sperm. ICSI leveled the playing field for male infertility with just a few moving sperm to help get the woman pregnant and we can use it when there is a previous vasectomy or production problem, just as we do with tubal ligation or bypass.
The ability to grow embryos in the lab has increased through the development of ICIS in 1995 which now allows us to treat in the middle of the process. The old way with standard insemination takes eggs retrieved in a culture dish and puts a sperm concentration in it in the same drop to fertilize. The problem is it didn’t work if there was a significant male- factor such as low sperm. ICSI leveled the playing field for male infertility with just a few moving sperm to help get the woman pregnant and we can use it when there is a previous vasectomy or production problem, just as we do with tubal ligation or bypass.
What About Lab Safety Protocols?
Today we are designed to assume optimal positions for survival and the growth of embryos, to protect patients, numerous protocols with the chain of custody of the sperm, eggs, embryos, labeled, only working with one person at a time, kept separately in parts of the incubator, media injection, pipe heads, quality control by manufacturers and the like. We regularly retest in our clinic with mice embryos to make sure they divide properly, logs that are kept for PH, temperature, the media, and ensure nothing’s expired. We also report to START and to the CDC reproductive health branch following the numbers and statistics of all IVF clinics in the nation. There are so much oversight and protective processes now.
Our 3 IVF labs (Greenville, Columbia, and Lowcountry) each have their own emergency natural gas-powered backup generator which is tested every week with monthly maintenance to allow with a loss of power to work for days and days because of natural gas. There are multiple alarm systems in the lab and monitoring things such as air quality, the PH, temperature, too warm or cold, gas mixture not right, liquid nitro cryopreservation tanks start warming, alarms and notifications start going off. The embryologists maintain these safeguards and protocols daily.
We’ve Come a Long Way with IVF Haven’t We?

We take IVF very seriously the processes, procedures, and policies to safeguard sperm, egg, embryos, everything in place for the right patients’ gametes and advanced techniques available to further safeguard with breakthroughs and advances in assisted reproduction technology that continues to evolve. For example, our incubators are so much smaller than the hold big box ones. These new incubators require less gases and are continuously monitored, for Ph, gas mix, temperature, and more. Imagine a refrigerator with 16 compartments and each has it’s one open and close with one dish for that patient. The older models were like college dorm refrigerators with three shelves. So we can safeguard even better with barcodes, color-coded tapes, names, and our instituted protocols. In less than 40 years since that first baby in 1978, we’ve come a long way and there are a lot of advances still to come. The ability to do genetic testing has been incredible, but our goal is to have the highest success rate possible while transferring the fewest embryos with only single babies at a time to reduce risk to mother and baby.
![]() PREG has 3 IVF Centers (Greenville, Columbia & Low Country) with offices in Asheville & Spartanburg.
PREG has 3 IVF Centers (Greenville, Columbia & Low Country) with offices in Asheville & Spartanburg.
866.725.7734